- Oak Brook:(630) 705-9999
- Chicago:(312) 920-8822
- Email:inquiry@vervecollege.edu
- Make a Payment
 Sign up
Sign up Login
Login- Home
- Programs
- Admission
- Resources
- ATI Entrance Exam Resources
- New E-Digital Library
- Refer a Friend
- School Newsletter
- Events
- Employers
- Job-Network
- Alpha Beta Kappa Candidates
- Verve College Library
- Graduation and Pinning Ceremony Photo Galleries
- Textbook Information
- Career Services
- Tutoring
- School Catalog
- FAQ
- Constitution Day Program
- Alumni
- Verve College Plans
- Financial Aid
- HEERF Reporting
- Satisfactory Academic Progress
- Apply For Financial Aid
- Net Price Calculator
- Return of Title IV Funds (R2T4)
- Financial Aid Office Code of Conduct
- Contact
- FAQs
- Verification Policy
- Vaccination Policy
- Student Right-to-Know Act
- Misrepresentation
- Information Security Program
- Academic Award Year
- Availability of Employee
- Cost of Attendance
- Health & Safety Exemption Requirement
- Students Rights and Responsibilities
- Leave of Absence
- Pell Formula
- Military Students
- Grants/ Scholarship Policy
- Contact Us
- Testimonials
- Blog
Is a Nursing Career Right For You?
Take The Free Quiz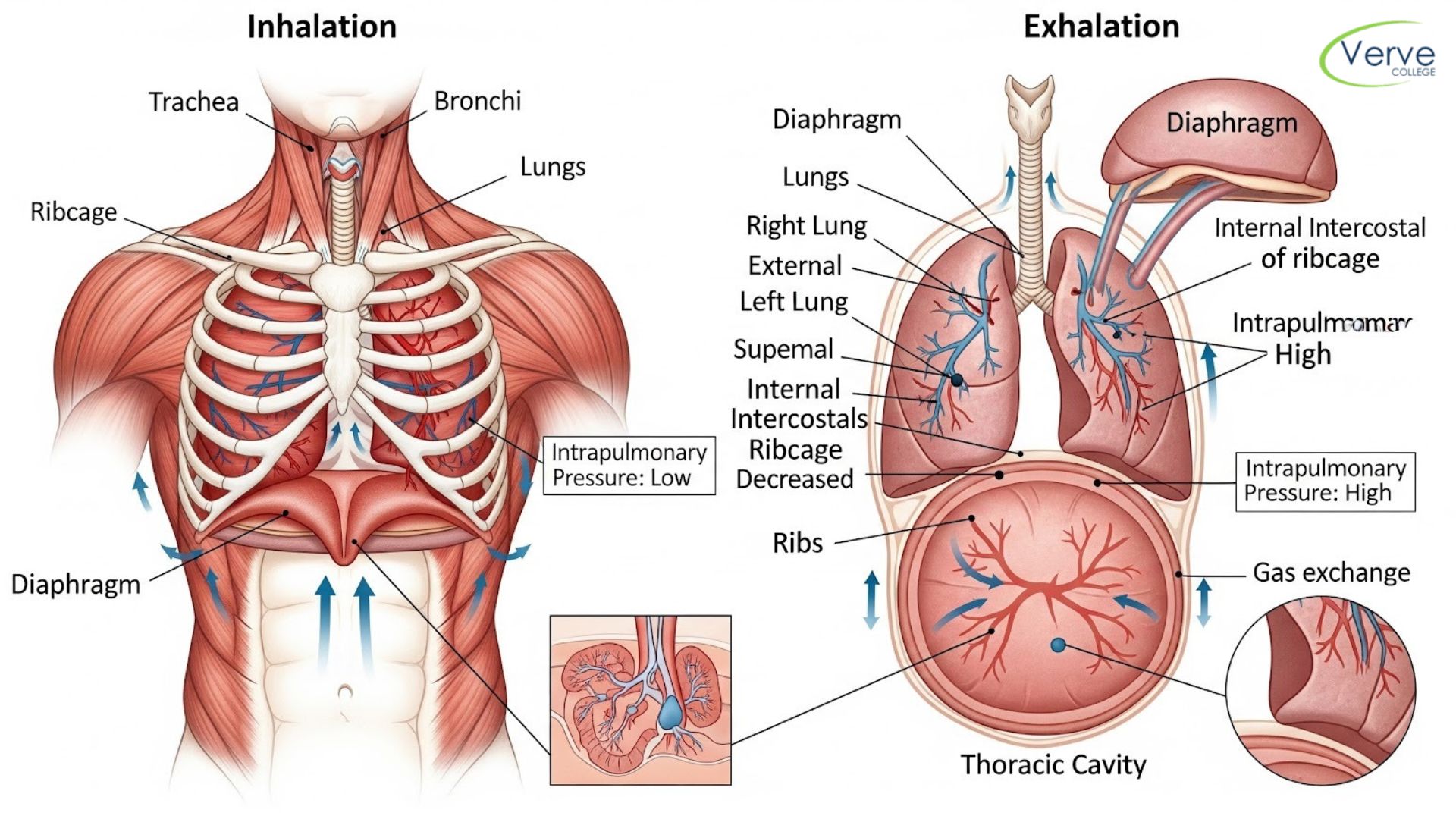
Breathing Mechanics for A&P Students (Without Overthinking)
Breathing Mechanics for A&P Students (Without Overthinking)
Let’s be honest: the human respiratory system is usually taught as a dry list of organs, but in reality, it’s a high-pressure masterclass in physics. For many nursing students, “Breathing Mechanics” is the hurdle where the excitement of healthcare meets the frustration of gas laws. You don’t need to be a physicist to understand how we inhale, but you do need to understand the relationship between volume and pressure. If you can grasp why a balloon expands, you can understand how a patient survives. This guide strips away the fluff and focuses on the mechanical “why” behind every breath.
Key Takeaways
- Pressure Gradients Rule: Air only moves when there is a pressure difference; it flows naturally from high-pressure zones to low-pressure zones.
- The Diaphragm is the Engine: By contracting and flattening, the diaphragm increases chest volume, which is the “mechanical trigger” for every breath you take.
- Boyle’s Law is the Secret: Understanding that Volume Up = Pressure Down is the only way to grasp how the lungs “suck” in air without actually being a vacuum cleaner.
- Inhalation Costs Energy: While breathing in is an active muscular effort, quiet breathing out (exhalation) is mostly a “free” passive process thanks to lung elasticity.
- Foundational Knowledge Wins: Mastering these mechanics early in an A&P prep course llinois prevents clinical burnout when you eventually manage complex respiratory patients.
Mastering the Mechanics: Breathing for the Future Nurse
The Diaphragm: The Only Muscle That Truly Matters (Mostly)
Section Key Takeaway: The diaphragm is the primary driver of respiration; its contraction increases thoracic volume, which drops internal pressure to draw air in.
Most people think we “suck” air in. We don’t. We create a vacuum and the atmosphere pushes air into us. When you sit in anatomy and physiology classes near me, you’ll learn that the diaphragm is a dome-shaped muscle that flattens out when it contracts.
Think of your chest as a syringe. When you pull the plunger back, the volume inside increases, the pressure drops, and fluid is pulled in. Your diaphragm is that plunger. If it doesn’t move, you don’t breathe. It’s that simple. For students balancing a job and education, our evening LPN programs emphasize these clinical realities: if a patient’s diaphragm is compromised, their “plunger” is broken.
Boyle’s Law: The Physics of Every Breath
Section Key Takeaway: Boyle’s Law states that pressure and volume are inversely proportional; as one goes up, the other must go down.
Physics is usually the part where students’ eyes glaze over, but stay with me. $P_1V_1 = P_2V_2$. In plain English: if you make a space bigger, the pressure goes down.
- Inhalation: Thoracic cavity expands $\rightarrow$ Volume increases $\rightarrow$ Intrapulmonary pressure drops below atmospheric pressure $\rightarrow$ Air rushes in.
- Exhalation: Thoracic cavity shrinks $\rightarrow$ Volume decreases $\rightarrow$ Intrapulmonary pressure rises above atmospheric pressure $\rightarrow$ Air rushes out.
Origin vs Insertion: Why This Topic Trips Up So Many Students
Why “Normal” Breathing is Passive?
Section Key Takeaway: Inhalation is an active process (requires energy), while quiet exhalation is passive, relying on the natural “snap-back” of lung tissue.
Nature is lazy. It loves to save energy. This is why quiet exhalation doesn’t require muscle contraction; it relies on elastic recoil. Your lungs are like rubber bands. Once you stop pulling them open (inhalation), they naturally want to snap back to their original size.
When a patient has a condition like emphysema, they lose that “snap.” They have to use extra muscles just to push air out. If you’re struggling to visualize this and provide the hands-on lab time to see these tissues in action before you ever hit the clinical floor.
Conclusion
Mastering breathing mechanics isn’t just about passing an exam; it’s about understanding the invisible forces that keep your future patients alive. When you stop viewing the lungs as balloons and start seeing them as a precision-engineered pressure system, the “aha!” moment happens. This fundamental shift in perspective turns rote memorization into clinical intuition, allowing you to recognize respiratory failure before it becomes a crisis.
At Verve College, we know that the transition from student to nurse requires more than just reading—it requires a deep, mechanical understanding of the human body. Our programs are designed to take these complex concepts and make them implementable in a real-world setting. Whether you are building your foundation in an A&P prep class or refining your clinical skills in our nursing labs, you are preparing for a career where “knowing the why” is what makes you an exceptional healthcare professional.
Frequently Asked Questions (FAQs)
Q: What happens if the pleural cavity is punctured? A: The vacuum is lost. This is called a pneumothorax. Without that negative pressure “suction” holding the lung against the chest wall, the lung’s natural elasticity causes it to collapse like a deflated balloon.
Q: Why do we use “accessory muscles” when we are short of breath? A: When the diaphragm isn’t enough to meet oxygen demands, muscles in the neck and chest (like the sternocleidomastoid) kick in to pull the ribcage even further up and out, creating a larger pressure drop for more air intake.
Q: Is exhalation always passive? A: No. During exercise or respiratory distress, “forced exhalation” occurs. This is an active process where abdominal muscles and internal intercostals contract to forcefully push air out of the lungs.
Q: Why does it feel harder to breathe at high altitudes? A: The mechanics of your lungs don’t change, but the atmospheric pressure drops. Since the pressure “pushing” air into your lungs is lower, the gradient is smaller, making it feel like you’re working harder for every sip of air.
Q: Is an A&P prep course really necessary before nursing school? A: If you want to enter a nursing program with clinical confidence rather than textbook confusion, yes. It builds the foundation so you aren’t stuck relearning basic physics while you’re supposed to be learning patient care.
Most Popular Blogs Posts

Glasgow Coma Scale Explained: A Practical…
July 29, 2026 Read More
Patient Education Strategies Every Future Nurse…
July 29, 2026 Read More
CMP vs BMP: What’s the Difference?
July 28, 2026 Read More
CBC Test Basics Every Nursing Student…
July 28, 2026 Read More