- Oak Brook:(630) 705-9999
- Chicago:(312) 920-8822
- Email:inquiry@vervecollege.edu
- Make a Payment
 Sign up
Sign up Login
Login- Home
- Programs
- Admission
- Resources
- ATI Entrance Exam Resources
- New E-Digital Library
- Refer a Friend
- School Newsletter
- Events
- Employers
- Job-Network
- Alpha Beta Kappa Candidates
- Verve College Library
- Graduation and Pinning Ceremony Photo Galleries
- Textbook Information
- Career Services
- Tutoring
- School Catalog
- FAQ
- Constitution Day Program
- Alumni
- Verve College Plans
- Financial Aid
- HEERF Reporting
- Satisfactory Academic Progress
- Apply For Financial Aid
- Net Price Calculator
- Return of Title IV Funds (R2T4)
- Financial Aid Office Code of Conduct
- Contact
- FAQs
- Verification Policy
- Vaccination Policy
- Student Right-to-Know Act
- Misrepresentation
- Information Security Program
- Academic Award Year
- Availability of Employee
- Cost of Attendance
- Health & Safety Exemption Requirement
- Students Rights and Responsibilities
- Leave of Absence
- Pell Formula
- Military Students
- Grants/ Scholarship Policy
- Contact Us
- Testimonials
- Blog
Is a Nursing Career Right For You?
Take The Free Quiz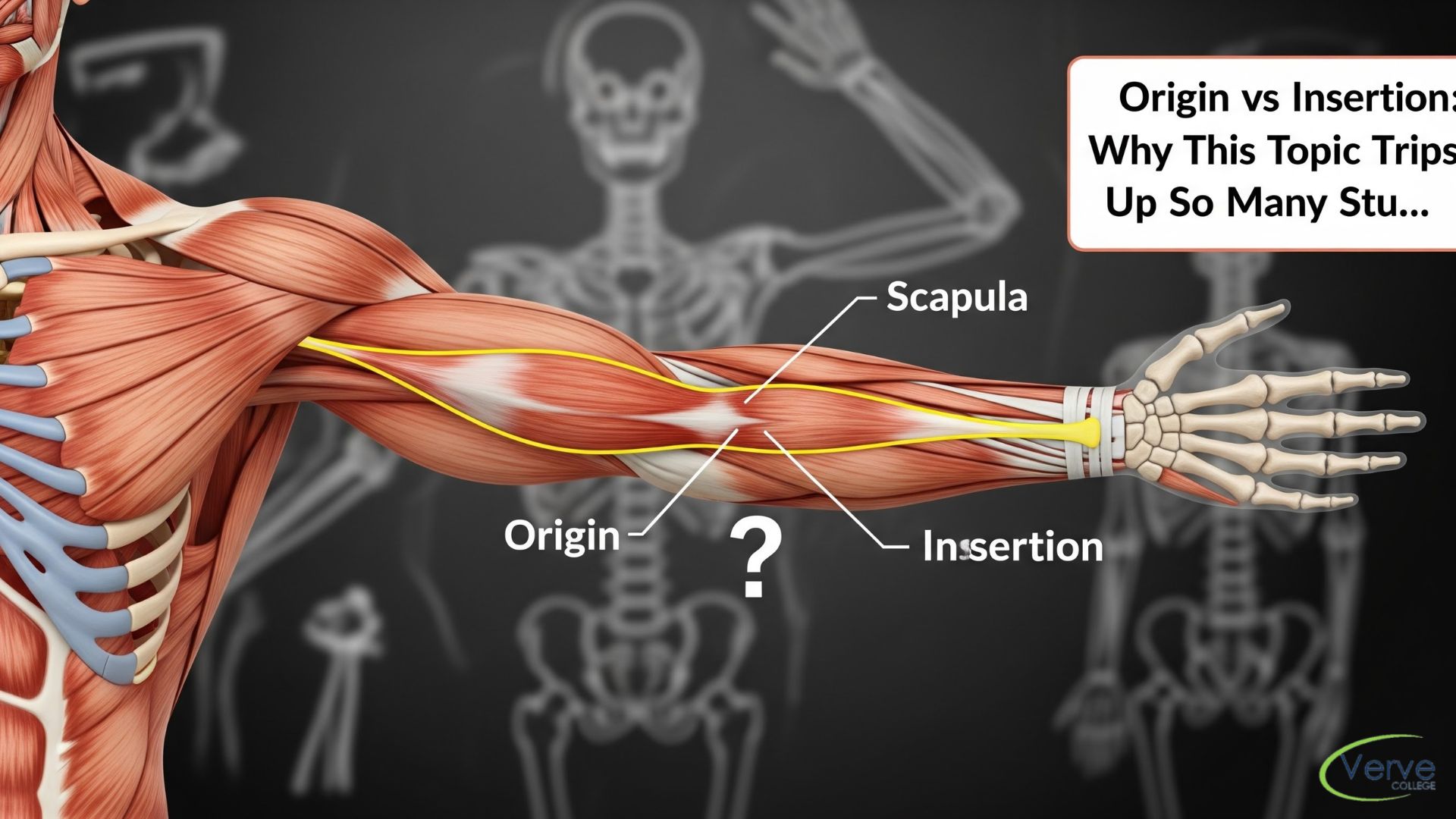
Origin vs Insertion: Why This Topic Trips Up So Many Students
Origin vs Insertion: Why This Topic Trips Up So Many Students
You are sitting in your anatomy lab, staring at a model of the human arm, and your brain freezes. You know the muscle. You know what it does. But when the exam asks for the origin versus the insertion, it feels like a high-stakes coin toss. Let’s understand the overview of Origin vs Insertion in short.
This isn’t just a “you” problem: it is a universal rite of passage for nursing students. The terminology feels arbitrary, the definitions seem to overlap, and under the pressure of a timed quiz, everything starts to look like a “fixed point.” Mastering this distinction is the difference between guessing your way through a musculoskeletal exam and truly understanding how the human body moves. If you find yourself searching for a high-quality anatomy and physiology course near me, it’s likely because these foundational concepts need more than just a textbook: they need a strategy.
Key Takeaways: The Cheat Sheet
- The Origin is the stationary anchor point, usually located proximally (closer to the center of the body).
- The Insertion is the “mover,” attached to the bone that actually moves when the muscle contracts.
- Functional Pull: Muscles always pull the insertion toward the origin; they never “push.”
- Proximity Rule: In the limbs, the origin is typically the attachment point closest to the torso, while the insertion is further away.
- Clinical Application: Knowing these points is critical for intramuscular injections, injury assessment, and patient rehabilitation.
Tug-of-War: Defining Origin vs. Insertion
Key Takeaway: The “Anchor vs. Action” Rule
Think of a muscle like a bungee cord: one end is tied to a tree (Origin) and the other to a person jumping (Insertion). The tree doesn’t move, but the person does.
To understand muscle attachments, you have to think in terms of stability and mobility. In the world of healthcare education, especially at the best nursing schools in Illinois, we emphasize that muscles never work in isolation: they pull.
The Anatomical Anchor: What is the Origin?
The origin is the attachment site that doesn’t move during contraction. It is the “stable” end. Traditionally, in the limbs, the origin is the most proximal attachment: meaning it is closer to the torso. When a muscle contracts, it pulls toward the origin. It is the foundation upon which the movement is built.
The Movable Feast: What is the Insertion?
The insertion is the opposite end. This is the attachment site on the bone that moves when the muscle shortens. Usually, the insertion is distal (further away from the center of the body). If you are flexing your bicep, the point where the muscle attaches to your forearm (the radius) is the insertion, because your forearm is the part doing the traveling.
Why the Confusion? Breaking the Mental Barrier
Key Takeaway: Context is King
Confusion happens because “fixed” is relative. To master A&P, you must visualize the movement, not just memorize a list of bones.
Most students trip up because they try to memorize origins and insertions as a list of “Point A” and “Point B.” This is a recipe for disaster. Human bodies are dynamic. While the origin is usually the fixed point, certain functional movements can make things look blurry.
However, for the sake of your boards and your clinical practice, the rule remains: Origin = Stationary; Insertion = Mobile. If you are struggling to visualize this, it might be time to look into nursing schools in chicago IL that offer hands-on, intensive preparatory support to get your fundamentals solid.
The “LPN Strategy” to Master A&P Concepts
Key Takeaway: Move Your Own Body
Don’t just read about the muscle: contract it. Physical movement creates “muscle memory” in your brain, making the origin and insertion intuitive.
If you want to survive a fast-paced nursing program, you need to stop studying like a philosopher and start studying like a clinician. When you look at a muscle, physically perform the action it’s responsible for.
- Locate the joint being crossed.
- Feel which bone stays still (that’s your origin).
- Feel which bone moves (that’s your insertion).
Conclusion
Above mentioned clearly about Origin vs Insertion. Origin and insertion shouldn’t be the reason you lose sleep. One stays, one goes. One is the anchor, one is the actor. Once you stop viewing them as vocabulary words and start viewing them as mechanical realities, the entire musculoskeletal system becomes a lot less intimidating. It is about visualizing the tension and the pull: once you see the “tug-of-war” in your mind’s eye, you’ll stop second-guessing yourself on exam day and start thinking like a seasoned professional.
If you’re ready to move beyond the basics and dive into a rigorous, supportive environment, it’s time to stop searching and start doing. Mastering these foundational concepts is the first step in a much larger journey. At Verve College, we specialize in taking these complex anatomical puzzles and turning them into the clinical intuition you’ll use every day on the floor. Your education shouldn’t just be about passing a test; it should be about building the certainty required to provide excellent patient care.
Frequently Asked Questions
- Can a muscle have more than one origin? Absolutely. Many muscles are “multi-headed.” For example, the biceps brachii has two origins (hence “bi”), and the triceps has three. They all eventually merge into a single insertion point to focus their power on moving one specific bone.
- Does the origin ever move instead of the insertion? In specific scenarios called “reverse muscle action,” the origin can move toward the insertion (like doing a pull-up where your torso moves toward your stable arms). However, for the sake of standard testing in any anatomy and physiology course near me, you should stick to the traditional rule: the insertion moves, the origin stays put.
- How do I remember which is which during a high-stress exam? Use the “Alphabet Rule” or the “Mobile Rule.” Insertion and “In motion” both start with the same idea. Or, remember that the Origin is the Off-limits point for movement. If you can identify the joint, the bone that crosses the joint to create the movement is always carrying the insertion.
- Why do some textbooks say the origin is always proximal? In the limbs, the origin is almost always the point closest to the trunk (proximal), while the insertion is further away (distal). This is a reliable shortcut for 90% of the muscles you will study in nursing schools in chicago il, but always double-check the specific functional movement to be sure.
- Why is this distinction so critical for practical nursing? Understanding where a muscle begins and ends isn’t just for anatomy buffs: it’s vital for identifying where to safely administer intramuscular injections and for accurately documenting patient mobility or musculoskeletal injuries. Accuracy in terminology ensures better communication within the healthcare team.
Most Popular Blogs Posts

What Is Systems Thinking in Nursing?…
July 8, 2026 Read More
How Organ Systems Work Together in…
July 8, 2026 Read More
Understanding Acid-Base Balance in Anatomy and…
July 7, 2026 Read More
What Is Perfusion in Nursing? A…
July 7, 2026 Read More